Injuries in Athletes of
National Handball Teams
Dimitris Hatzimanouil1,
Nikos Oxizoglou2, Aggelos Kanioglou1, Kostas
Manavis3, Stefas Eleftherios3
1Department
of Physical Education and Sports Science
Aristotle
University of Thessaloniki, Greece
2Department
of Physical Education and Sports Science at Serres
Aristotle
University of Thessaloniki, Greece
3Department
of Anatomy, Medical School
Aristotle
University of Thessaloniki, Greece
CORRESPONDENCE:
Hatzimanouil
Dimitris
Glinou
34 street
T.K.
54352 Pilea
Thessaloniki
Greece
Tel:
(+30) 2310925624
Fax:
(+30) 2310925624
E-Mail:
xatjiman@phed.auth.gr
|
ABSTRACT
Team
handball includes movements that produce
stress to the myoskeletic system and consequently injuries. The aim of
the study was the recording of injuries, as these are recorded by the
athletes themselves. The sample constituted 32 athletes members of
national teams of men and juniors aged 19 years or more. Each athlete
completed a questionnaire relative to the injuries that he
suffered in the previous 24 months. From the results it appeared that
the majority of athletes did not use protective equipment. The
frequency of injuries was high (46.8%) corresponding for 0.7 injuries
in 1000 athletic hours. Most injuries presented the wings and the
pivots. The severity of the injuries in their majority was moderate
and serious (77.3%). The injuries concerned mainly the ligaments of
the lower limbs (78.3%). The main cause of the injuries was violent
contact with opponents (57.1%) during training (69.6%). Most players
followed conservative treatment (68.2%), while a small percentage of
these injuries relapsed. The athletes that had presented less
injuries in the past return to athletic activity sooner in contrast
to those with more injuries. More severe injuries presented in those
that had not followed the preseason program. Deductively this
competition level demonstrates high frequency of severe injuries,
while the need of further research in a bigger sample is obvious.
Key
words: Injuries, musculoskeletal system, men’s health.
|
INTRODUCTION
In sports that require
contact with opponents, there
exists a bigger probability of injury in contrast to sports without
body contact (American Association of Oral & Maxillofacial
Surgeons, 1999; Kujala, Taimela, Antti-poika, Orava, Tuominen &
Myllynen, 1995). Moreover, sports of contact also have a big risk of
injury for both genders (Loes and Goldie, 1988). Some of those carried
out indoors are characterized by intense contact and
high number of jumps (Backx, Beijer, Bol & Erich, 1991). In this
category belongs the sport of handball, which is spread worldwide and
has been part of the Olympic Games since 1972 (Pokrajac, 1989). This
particular sport includes movements that produce stress to the
myoskeletic system and consequently injuries (Andren-Sandberg, 1994;
Loes and Goldie, 1988; Tyrdal and Bahr, 1996; Werner and Plancher,
1998). Therefore, the requirements and the particularities of this
sport, as for example the frequent and intense contact with the
opponent players,
often leads to injuries (Andren-Sandberg, 1994; Asembo and
Wekesa, 1998; Wolf et al. 1974).
Hoeberigs, van Galen, and
Philipsen (1986),
suggested that each sport should have its own model of injuries,
which can be more or less specialised. The knowledge of this model,
can be very important for the planning of medical care that perhaps
needs to be given and is useful to define the most important
causative factors of injuries in handball. The necessity of knowledge
of this model that concerns injuries in this sport particularly,
appeared also from the study of Nielsen and Yde (1988), in which it was
documented that the knowledge of athletic injuries and their
rehabilitation was poor, for both athletes and
coaches. Except for the factors that are
related to specific requirements of the particular sport, there also
exist various exogenous factors, such as the erroneous application of
regulations, the material of the court surface and the dimensions of
the court that lead to injuries (Boden, Griffin & Garrett, 2000;
Jorgensen, 1984; Seil, Rupp, Tempelhof & Kohn, 1997).
One particular
characteristic of handball is the
high frequency of injury not only in adults but in junior athletes
too (Loes and Goldie, 1988; Tittel, Schaetz & Hagen, 1974; Wolf
et al, 1974). This conclusion is reached by a number of scientific
publications (Backx, Beijer, Bol & Erich, 1991; Bak and Koch,
1991; Engebretsen, Gruntvedt & Bredland, 1993; Fagerli, Lereim
&
Sahlin, 1990; Hoeberigs et al., 1986; Sorensen, Larsen & Rock,
1996; Yde and Nielsen, 1990). The above mentioned injuries lead, many
times, to the individuals being admitted to hospital with injuries of
high severity
that require medical care (Jorgensen, 1984; Hoeberigs et al., 1986;
Maehlum and Daljord, 1984; Menquy, Guillou & Condamine, 1999).
The sustained injuries appear to be of high severity because the
majority of athletes are absent from training sessions for more than
a week (Biener and Perka, 1980; Lindblad, Jensen, Terkelsen,
Helleland & Terkelsen, 1993; Lindblad, Hoy, Terkelsen, Helleland
& Terkelsen, 1992; Nielsen and Yde, 1988). Asembo and Wekesa
(1998), suggest that injuries in handball are inevitable. They
also suggest that for these specific injuries measures of prevention,
treatment and rehabilitation should be taken. Adamczewski
(1999), also suggests that for the reduction in frequency of such injuries,
preventative actions are recommended. The Wolf et al. (1974), report
that the main actions of prevention are determined by the observation
of injury factors.
If we consider that almost
50% of handball
players sustain at least one injury throughout a year (Hoeberigs et
al, 1986), that a percentage of the injured athletes are hospitalized
and that the majority of these athletes are absent from training
sessions for more than a week and finally that a percentage of these
athletes abandon the sport because they could not recover from the
injury (Lindblad et al, 1993), we understand that injuries in
handball constitute an important issue concerning this particular
sport. The cause of injuries in each sport can differ between
different subgroups of the athletes’ population. Different
subgroups of the athletes' population in each sport, also need different
prevention programs, so that the highest frequency and severity
reduction of particular injuries is achieved. Therefore, scientific
research should be specialised, so that the groups at high risk are
ascertained and independent variables for forecasting injuries are
defined for each subgroup separately. The results of such studies can
provide effective precautionary measures and prevention programs. It
is desirable that such research include similar subgroups for the
determination of injuries and should be based on epidemiologic and
methodological principles (Inklaar, 1994).
Deductively, it is obvious
that while the
interest for the sport of handball is steadily increasing, there is
absence of research via which we would generate precious information
and reliable data on factors that determine the reduction
of injuries in national team level. Via research, prevention measures
will be upgraded. Moreover there is lack of research data about
injuries of handball players of national teams that evolve after a
long-lasting period of participation. Lack of data and research that
concerns this particular subject gave birth to the present study.
Thus, the aim of this study was the recording of injuries that
occurred in Greek national teams' handball players aged 19 years or
more, with the final objective to become a useful tool in finding those
measures of prevention that will contribute to future injury
reduction.
MATERIALS
AND METHODS
Sample
The total sample of
the study consisted of 32 handball players who were in Greek national
teams of juniors
and men. All athletes were regular participants of the teams. Junior
athletes participated in preliminary European championship and men
participated in the pre Olympic preparation.
Research tools
All athletes were given a
self-reported
questionnaire developed specifically for this
research. The questionnaire was related to
the injuries the players had suffered during
their involvement with the sport within the
period of the last 24 months. An injury was
defined as an accident sustained during
practice or competition, which led to a
medical problem (e.g., pain, disability) and
prevented participation in training sessions or games for at least
one day beyond the date of occurrence (Gibbs, 1993; Hodgson, Standen
and Batt, 1998). More
specifically, at the beginning of the questionnaire each player was
required to give information and data on
personal characteristics such as age, weight, height and his history
of athletic activity and participation. In addition, each player gave
further information about warm up exercises, prophylactic
equipment, stretching exercises and technical training. In
the main part of the questionnaire, information was required on
injuries which the players had sustained during the last two years.
For instance, the incidence, severity (injuries were graded into four
categories of severity): mild (absence
from practice less than 1 week), moderate (1-2 weeks absence),
serious (2-4 weeks absence), and severe (more than 4 weeks absence)
(Seil, Rupp, Tempelhof and Kohn, 1998), the percentage of
players who had to be hospitalized,
localization, type and mechanism of injury,
time (that is,
during training or at a match), type of treatment, and
relapse of the injury. Finally, information was asked about various
environmental factors, such as the surface of the field, the soles of
the player’s shoes as well as the place where the injuries
occurred.
Procedure
The questionnaires were
suitably formed and
were completed by each player separately during the visit made by the
researchers at one of each national team training sessions. The
completion of the questionnaires was done during Junior's European
Championship and Men’s Balkan Championship. Participation in the
study was voluntary. If an injury was listed, more questions had to
be answered regarding the severity, localization, time (that is,
during training or at a match) and relapse. The researchers were
present to answer any questions posed by the athletes. There was a
100% response from the questionnaire. In total, 32 questionnaires
were completed. All injuries reported concerned sport injuries and
not those related to overuse syndromes. Nicholas and Hershman (1990),
state that sport injury is an acute myoskeletic injury, related to an
accident which happened in scheduled matches or training sessions and
which results in the absence of a player from at least one match or
training session.
In the present study
handball players were
asked to complete a self-reported questionnaire. Therefore an issue
can be raised regarding its reliability. It should be underlined that
none of the scientific articles that were used as a reference for the
research confirmed the reliability of the administered questionnaire.
It is possible that the contradictory results which are frequently
found in the literature, regarding sport injuries, stems from tools
of low reliability. Future studies should attempt to clarify this
issue. The results of the
present study should be viewed while taking into account the above considerations.
Statistical Analysis
The mean, the standard
deviation, the frequency
of the values of each variable and their percentage were considered in the descriptive
statistical analysis of the
data. In the deductive
statistic analysis Kruscal Wallis' and Mann Whitneys' scale was used
to define the interaction between frequency and severity of injuries
and all other variables.
RESULTS
Descriptive statistics
From the statistical
analysis of the
results concerning the players’ personal characteristics the
average age was 23.1±3.9 years. The
average weight was estimated at 84.4±16.87 kg and height at
188±7.19 cm. The average training age was 10.9±3.54
years, with 6.3±1.4 average training sessions per week. All
the players executed warm-up exercises. The
use of prophylactic equipment was 43.8% for the total number of
players. This prophylactic equipment was
used exclusively for the protection of the joints and not for
rehabilitation or treatment reasons. Moreover, all players were
physically fit and were not involved in rehabilitation or treatment,
which meant they were ready to participate in a game. Stretching
exercises were executed in two ways: at the warm-up period and after
training or games. At the warm-up period the percentage was 90.9%.
After training or games the percentage was 72.7%. The majority of
players (81.3%) reported the use of technical training, which helps
to avoid injuries due to poor technique.
Our findings also revealed a
high incidence of
injuries for the total number of team handball players. Fifteen out
of all players (46.8%) had treatment for at least one injury during
the previous two years. Specifically these
athletes had a frequency of injury of 0.7 per 1000 hours of reported
athletic activity. From the athletes with injuries, 11 (73.3%) had
suffered an injury, 3 (20%) had suffered two injuries and 1(6.7%) had
suffered above two injuries in a 2 years period. Moreover, the most
injuries presented the line players (Table 1).
Table1. Number of injuries and
field position.
|
FIELD POSITION
|
NUMBER OF ATHLETES
|
ATHLETES WITH INJURY
|
%
|
|
GOALKEEPERS
|
7
|
2
|
6.25
|
|
WING
|
9
|
4
|
12.5
|
|
CENTRAL BACKCOURT
|
3
|
2
|
6.25
|
|
BACKCOURT
|
7
|
3
|
9.3
|
|
PIVOT
|
6
|
4
|
12.5
|
|
TOTAL
|
32
|
15
|
46.8
|
Regarding the severity of
injuries, these were
9.1% of soft form (absence from trainings for at least one week),
36.4% of moderate form (1-2 weeks absence), 40.9% of serious form
(2-4 weeks absence) and 13.6% of severe form (more than 4 weeks
absence). See Figure 1.
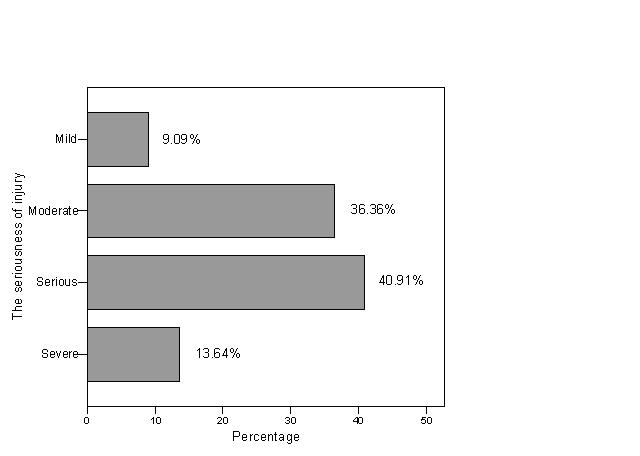
Figure 1, Severity of injuries
As for the frequency of
injuries, the results
pointed out that the athletes who suffered a single injury in the past,
came back sooner to the prior state of athletic activity, in contrast
to those who had suffered two or above injuries. Mann Whitney U=2.00,
p=.027.
Severity of injuries:
As for the severity of an
injury, it appeared
that those that had not followed the preseason program presented
higher severity of injuries.
H=10, p=.019. It appeared also that in the training sessions we had
more serious injuries in contrast to games. H=7.55, p=.05. The
athletes that had more serious form of injuries followed a surgical
treatment. H=10.47, p=.01. Finally, it appeared that the athletes
that had more serious form of injuries needed more days for their
comeback to athletic activity. H=13.29, p=.00.
DISCUSSION
A percentage of athletes
56.2% did not use protective
equipment. This result correlates with that of Tsigilis and
Hatzimanouil (2005), in only that the 41.7% of all handball players
of the Greek first league made use of protective equipment. In
handball intensive precautionary measures should be applied not only
during games, but also during training sessions (Wolf et al, 1974).
As it appears from the research of Dirx, Bouter and Geus (1992),
protective measures are of high significance for the reduction of
injuries. Biener and Fasler (1978), recommend to the high
risk group of athletes particularly those that had a history of
injuries in the ankle joint and in the lower limbs, to consider as a
standard procedure protective taping or other protective measures in
the above-mentioned joints. The same researchers recommend the use of
kneecaps and elbow caps. Biener and Perka (1980), report as a
protective measure taping before training session, but also the use
of other protective equipment that will minimize the risk of
injuries. Adamczewski (1999), supports that taping has a lot of
advantages.
The majority of athletes
used
stretching exercises in the warm-up and also after the end of the
training session or the game. As Aronen (1995 & 1991) reports,
stretching exercises before and after the training session, is a
measure of high significance for the prevention and reduction of
injuries. Of course, Bradford (2000) reports that the stretching
exercises should be continued after an injury as a measure to prevent
relapse.
Moreover, most athletes
followed a program of
technique exercises in order to avoid injuries as a consequence of
bad technique application. As Aronen supports (1995), errors in
technique is a cause of injuries. Ehrich and Gebel (1992) propose
that the technique exercises should be of special stress, in order to
correspond to the requirements of a game. The most common case of
erroneous technique is that of the reception of the ball, which
causes injuries
(disarticulation) in fingers
(Aronen, 1991; Biener and Fasler, 1978 Taillandier, Quignard and
Pilardeau, 1990).
According to the results it
appears that 15
out of 32 players (46.8%) had suffered at least an injury during the
past 2 years and this points to a high incidence of injuries in this
particular group of athletes. These results correlate with those of
Tsigilis and Hatzimanouil (2005) who examined handball players of the
Greek first league. These particular athletes presented a frequency
of injuries of 0.96 per 1000 hours of reported (games and trainings)
athletic activity. The results that concern the incidence of athletes
that suffered two or more injuries, correlate with those of
Hatzimanouil et al. (2005), who examined Greek handball players of
different game level and found that the majority of athletes suffered
a serious injury in the past two years.
The results of the present
study concerning
field position and occurence of injury correlates with those of
Tsigilis and Hatzimanouil (2005) as well as Olsen, Myklebust,
Engebretsen, and Bahr (2006), who found that players playing the
field position of pivot and those playing the field position of wing
had the most injuries. This is logical because line attack players
have more frequent contact with opponent players who try to protect the
line. Moreover pivot always takes part in handgrips with the opposing
players when he catches the ball while the wings are the first players
who
take part in (individual or team) fast break thus very fast movements
are necessary.
The results of the present
study concerning
the severity of injuries, differ from those of Junge et al. (2006),
and Langevoort, Myklebust, Dvorak and Junge (2006), who examined
injuries during the 2004 Olympic Games in Greece and World cups and
found that most injuries resulted in abstinence from 0 days to a
week. The above-mentioned researchers examined and took into
consideration the injuries for the actual championships and did not
examine these athletes for a long-lasting period. Moreover in the
present study, an important percentage needed hospitalization. This
declares that some injuries require immediate hospital care.
Furthermore the rate of hospitalization correlates with the results
of Hatzimanouil et al. (2005), who analyzed injuries of handball
players in teams of different game level.
With regard to the
localisation and the type of
injuries, the results of this study correlate with those of Benito
(1999), who examined handball players of the national team of men of
Spain and found that the majority of injuries were located in lower
limbs and concerned ligaments and articulars injuries. The same
conclusions were made by Junge et al. (2006), and also Langevoort
et al. (2006), who examined handball players of national teams in
various championships and found that most injuries were located in
the lower limbs. The same researchers report that ligament injuries
were of high frequency. The cause of the majority of injuries was
contact with an opponent. These results correlate with those of
Langevoort (2003), Schulz, Henke and Heck (2005), the Junge et al.
(2006) and Langevoort et al. (2006) who report that the majority of
injuries is due to contact.
The 69.6% of injuries in the
last two years
were sustained during training sessions. These results do not
correlate with those of Schulz et al. (2005),
Andren-Sandberg (1994), Myclebust, Maehlum, Holm and Bahr (1998),
Myclebust, Maehlum, Engebretsen, Strand and Solheim (1997), Nielsen
and Yde, (1988), Retting, 1998, Seil et al. (1998),
Seil, et al. (1997) and Tyrdal and Bahr
(1996), who however examined athletes of national championships and
not international handball players. Probably this happens because of
the small participation of the athletes in official games during the
last two years. The majority of the athletes followed conservative
treatment and only certain cases of injuries needed surgical
treatment. This correlates to Benito's (1999) results.
Moreover, the results of the
study that
concern the relapse of injuries that were reported by the athletes,
correlate with those of Nielsen and Yde (1988), who however examined
handball players in teams of associations. Although most injuries
were sustained on a wooden floor, according to Olsen, Myklebust,
Engebretsen, Holme and Bahr (2003), the type of floor is not related
to the increase of the number of injuries to men handball players,
while on the contrary it is related with the occurrence of injuries
in women handball players. Moreover, the results showed that the
majority of players were wearing suitable footwear. Seil et al.
(1998), support that the combination of flexible floor and soles of
the shoes, possibly is the responsible factor for frequent
complications at lower limbs. Jorgensen (1984), suggests that for
handball players a shoe with 'high cut' should be preferred and
that the soles of the shoes should correspond in the different floors
that an athlete can meet. This footwear should protect the ankle and
its sole should have a moderate friction with the floor. This is
proposed for the reason that footwear with 'low cut', while they
give bigger acceleration, leave the ankle exposed. Missteps also
are due to very small or very large friction, while suitable
footwear constitute an important measure to prevent injuries
(Andren-Sandberg, 1994; Biener
& Perka,
1980; Quinn, Parker, de Bie, Rowe & Handoll, 2000; Tittel
et al.,
1974).
CONCLUSIONS
Deductively, handball players of national
teams of men and juniors do not use protective equipment for
joints, and they present a high frequency of severe injuries.
The players playing the field position of pivot and wing present most
injuries, which are located in lower limbs and they mainly concern
joints. They are caused after contact with the opponent during
training session, they heal after conservative therapy, while some
relapse in a small percentage. The flooring, the footwear of athletes
as well as the characteristics of playfields at the time of injuries
were found to be appropriate. The frequency of past injuries relates
to the time that is required in order for the athlete to return to
prior athletic activity, while the severity of the injuries relates
to the attendance of season and preseason training schedule.
REFERENCES
Adamczewski,
A. (1999). Tapen-Einfrach Fuer Alle. World
handball magazine (Basel), 2: 50-53.
American Association of Oral and Maxillofacial
Surgeons. (1999). (AAOMS). Illinois, U.S.A.
Andren-Sandberg, A. (1994) Injuries in team
handball. In Renstrom P. A. F. H. Clinical
practice of sports injury prevention
and care. Blackwell Scientific
Publications, Oxford, pp. 354-359.
Aronen,
J. (1995). Handball injuries: prevention and treatment. Handball,
45(3):
56-57.
Aronen,
J. (1991). The spectrum of handball
injuries. Sports Medicine Digest,
13(4):
1-3.
Asembo, J.M. & Wekesa, M. (1998). Injury
pattern during team handball in East Africa. East African Medical
Journal, 75(2):
113-116
Backx, F.J.G., Beijer,
H.J.M., Bol, E. & Erich, W.B.M. (1991)
Injuries in high-
risk persons and high-risk
sports. A longitudinal study of 1818 children. American
Journal of Sports Medicine,
19:
124-130.
Bak,
K. & Koch, J.S. (1991). Subtalar
dislocation in a handball player. British
Journal of Sports Medicine,
25(1):
24-25.
Benito, J.J.M. (1999). Injuries in Spanish
handball. I.H.F. Periodical, 1: 42-44.
Biener, K. & Perka, D. (1980). Portrait of
the female handball player in sport medicine. Deutsche Zeitschrift fuer Sportmedizin,
31: 316-XII.
Biener, K. & Fasler, S. (1978).
Sportunfalle, Epidemiologie und Pravention. Verlag Hans Huber,
Bern Stuttgart-Wien, pp. 97-105.
Boden,
B.P., Griffin, L.Y. & Garrett W.E. (2000). Etiology
and prevention of noncontact ACL
injury. The physician and
Sportsmedicine, 28(4): 53-60.
Bradford, S. (2000). Common Sports Injuries. In
R. Rakel (Ed.), Conn’s Current Therapy 2000.
W.B. Saunders Company, St.
Louis, pp. 975-978.
De
Loes, M. & Goldie, I.
(1988) Incidence rate of injuries during
sport activity and physical exercise in a rural
Swedish municipality. Int. J. Sp. Med.,
9 :
461-467.
Dirx,
M., Bouter, L.M., de Geus, H. (1992). Aetiology
of handball: a case control study. British
Journal of Sports Medicine, 26:
121-124.
Ehrich,
D. & Gebel, R. (1992). Training
of rehabilitation after sports injuries. SALTO,
Thessaloniki, pp. 42-46.
Engebretsen,
L., Gruntvedt, T. & Bredland, T. (1993). A
prospective, randomized study of three surgical techniques
for treatment of acute ruptur. Tidsskr
Nor Laegeforen, 113:
952-954.
Fagerli, M., Lereim, I. & Sahlin, Y.
(1990). Injuries in handball players. Tidsskrift for den norske Laegeforening, 110(4):
475-478.
Gibbs, N. (1993). Injuries in professional
rugby league: A three-year prospective study of the South Sydney
professional rugby league football club. Am.
J. Sports Med., 21:
696-700.,
Hodgson,
P. L., Standen, P. J. & Batt, M. E. (1998). Effects
of seasonal change in rugby league
on the incidence of injury. Br. J.
Sports Med, 32: 144-148.
Inklaar, H. (1994). Soccer injuries. Part II:
aetiology and prevention. Sports medicine, 18(2): 81-93.
Jorgensen,
U. (1984). Epidemiology of injuries in
typical Scandinavian team sports. British Journal of Sports
Medicine, 18(2):
59-63.
Junge, A., Langevoort, G., Pipe, A., Peytavin,
A. Wong, F., Mountjoy, M., Beltrami, G., Terrell, R., Holzgraefe, M.
Charles, R. & Dvorak, J. (2006). Injuries in team sport tournaments during the 2004
Olympic Games. The
American Journal οf
Sports Medicine, 34(4):
565-576.
Hatzimanouil, D., Oxizoglou, N., Sikaras, E.,
Hatzimanouil, A., Koronas, K., Tsigilis, N. & Abatzides, G.
(2005). Factors related to the incidence and severity of injuries in
team handball. Journal of Human Movement
Studies,
48: 335-351.
Hoeberigs,
J., van Galen, W. & Philipsen, H. (1986). Pattern
of injury in handball and comparison
of injured versus non injured
handball players. International Journal Sports Medicine, 7:
333-337.
Langevoort,
G., Myklebust, G., Dvorak, J. & Junge, A. (2006). Handball
injuries during major
international
tournaments. Scand. J. Med. Sci. Sports,
(Online Early Articles),
doi:10.1111/j.1600-0838.2006.00587.x.
Langevoort,
G. (2003). Euro
2002 / Denmark
Injury report analysis. I.H.F.
Periodical, 1:217-219.
Lindblad, B., Jensen, K., Terkelsen, C.,
Helleland, H. & Terkelsen, C. (1993). Handball injuries. An epidemiological and socioeconomic
study. Ugeskr Laeger, 155(45):
3636-3638.
Lindblad, B., Hoy, K., Terkelsen, C.,
Helleland, H. & Terkelsen, C. (1992). Handball injuries. An
epidemiologic and socioeconomic study. American
Journal of Sports Medicine,
20(4):
441-444.
Maehlum,
S. & Daljord, O.A. (1984). Acute sports
injuries in Oslo: a one-year study. British
Journal of Sports Medicine,
18(3): 181-185.
Menquy, F., Guillou, M.A. &
Condamine, J. (1999). Sports accidents: a
prospective study
in 972 emergency cases
over a 3-month period. Journal de
traumatologie du sport, 16(3):
171-181.
Myclebust,
G., Maehlum, S., Holm, I. & Bahr, R. (1998). Aprospective
cohort study of anterior cruciate
ligament injuries in elite
Norwegian team handball. Scandinavian Journal of Medicine and
Science in Sports, 8(3): 149-153.
Myclebust, G., Maehlum, S., Engebretsen, L.,
Strand, T. & Solheim, E. (1997).Registration
of cruciate ligament injuries in
Norwegian top level team handball. A prospective study covering two
seasons. Scandinavian journal of medicine and science in sports,
7(5): 289-292.
Nicholas, J. & Hershman, E. (1990). The
lower extremity and spine. The CV Mosby Company, St Louis.
Nielsen,
A. & Yde, J. (1988). An epidemiological
and traumatologic study of injuries in handball. International journal of sports
medicine, 9(5): 341-344.
Kujala, U.M., Taimela, S., Antti-Poika, I.,
Orava, S., Tuominen, R., & Myllynen P. (1995). Acute injuries in
soccer, ice hockey, volleyball, basketball, judo, and
karate: analysis of national registry data.
British
Medicine Journal,
311(7018):
1465-1468.
Olsen,
O. E., Myklebust, G., Engebretsen, L., Bahr. R. (2006). Injury
pattern in youth team
handball: a comparison
of two prospective registration methods. Scand.
J.
Med. Sci. Sports, 16: 426–432
Olsen,
O. E., Myklebust, G., Engebretsen, L., Holme, I. & Bahr. R.
(2003). Relationship between floor type and risk of ACL injury in
team handball. Scand. J. Med. Sci. Sports, 13: 299–304.
Pokrajac, B. (1989) The Development of
Handball. Proccedings of international
symposium of I.H.F., Portugal, pp. 152-180.
Quinn
K., Parker P., de Bie R., Rowe, B. & Handoll H. (2000).
Interventions for preventing ankle ligament injuries. Cochrane
Database System Review, 2: cd000018.
Retting, A.C. (1998). Hand and wrist injuries.
Clinics in Sports Medicine, 17(3): 401-406.
Schulz, D., Henke, T. &
Heck. H. (2005). Prevention strategies in
professional handball
Br. J. Sports Med., 39:
401.
Seil, R., Rupp, S., Tempelhof, S. & Kohn,
D. (1998). Sports injuries in team handball: a one year prospective study in sixteen men’s
senior teams of
superior nonprofessional
level. American journal of sports
medicine, 26(5): 81-687.
Seil,
R., Rupp, S., Tempelhof, S. & Kohn, D. (1997). Injuries
during handball. A comparative retrospective
study between regional and upper league teams. Sportverletzung
Sportschaden, 11(2):
58-62.
Sorensen,
L., Larsen, S. & Rock, N. (1996). The
epidemiology of sports injuries in school aged children. Scandinavian journal of
medicine and science in sports, 6(5): 281-286.
Taillandier,
C., Quignard, M. & Pilardeau, P. (1990). Hand
injuries in handball and handball training.
Cinesiologie,
29(131):
141-146.
Tittel, K., Schaetz, P. & Hagen, D. (1974).
Zur Atiologie, Diagnostik, Therapie und Prophylaxe von Verletzungen
und Fehlbelastungsschaden bei Hallenhandballspielern. Medicine
und Sport, 2:
46-57.
Tsigilis, N. & Hatzimanouil, D. (2005).
Injuries in handball: Examination of the risk factors. European Journal of Sport Science,
5 (3): 137-142.
Tyrdal, S. & Bahr, R. (1996) High
prevalence of elbow problems among goalkeepers
in European team handball-‘handball
goalie’s elbow’. Scandinavian Journal of
Medicine and Science in
Sports, 6: 297-302.
Werner, S.L. & Plancher,
K.D. (1998) Hand and wrist injuries.
Biomechanics of wrist
injuries in sports, 17(3):
407-420.
Wolf, G., Tittel, K., Doscher, I., Luck, P.,
Hierse, B., Kiess, Chr., Lippold, G., Tetzlaff, B., Kohler, E. &
Schaetz, P. (1974). Statistische Analyse uber Ursachen,
Lokalisationen und
Arten haufiger bei
Training und Wettkampf aufgetretener Verletzungen und
Fehlbelastungsschaden im Hallenhandball. Medicine
und Sport, 3:
77-80.
Yde,
J. & Nielsen A. (1990). Sports injuries
in adolescents’ ball games: soccer, handball and basketball. British Journal of Sports
Medicine, 24(1): 51-54.